Does Routine Urinalysis Screening Benefit Asymptomatic Adults?
The Short Answer: No.
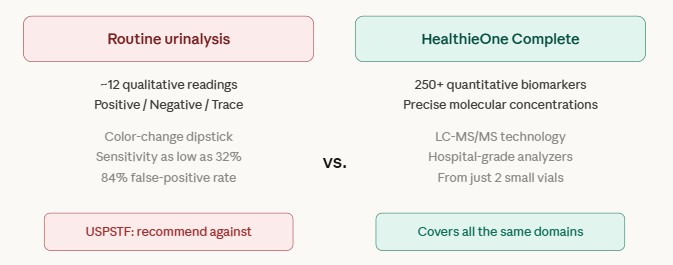
Multiple major medical organizations and evidence-based guidelines recommend against routine urinalysis screening in asymptomatic adults. The evidence is clear and consistent. At HealthieOne, our CLIA-certified, CAP-accredited laboratory routinely processes samples for institutional clients across all specimen types, including blood, urine, tumor, CSF, saliva, tissue, and other body fluids. We do not include routine urinalysis in HealthieOne Complete for direct-to-consumer testing for the reasons outlined below.
U.S. Preventive Services Task Force (USPSTF): Grade D Recommendation (Recommend Against)
The USPSTF, the gold standard for evidence-based screening recommendations in the United States, gives routine urinalysis screening in nonpregnant adults a Grade D recommendation, meaning they recommend against it. In their 2019 recommendation statement published in JAMA, the USPSTF concluded: "The USPSTF concludes with moderate certainty that screening for and treatment of asymptomatic bacteriuria in nonpregnant adults has no net benefit" [1].
The Task Force further stated that "the presence of asymptomatic bacteriuria has not been shown to increase the risk of adverse health outcomes among nonpregnant persons" [1]. The known harms of screening, they found, include "adverse effects of antibiotic use and changes to the microbiome" [1].
Peer-Reviewed Evidence: No Clinical Impact in Asymptomatic Adults
A 2021 peer-reviewed study published in Antimicrobial Stewardship & Healthcare Epidemiology examined the widespread use and misuse of urinalysis in clinical settings. The authors, from Duke University and Ascension Health, found that "routine urinalysis screening is a surprisingly common practice, used in ~25% of emergency department visits, but does not directly impact decisions of care" [2].
The study concluded that "even though routine urinalysis testing (ie, screening) is presumed to help detect urinary tract malignancy, renal disease, and diabetes, these diseases are rare in young asymptomatic persons, making false-positive and incidental findings more likely" [2]. The authors specifically stated: "An annual urinalysis is not warranted for screening asymptomatic individuals without major risk factors for bladder cancer” [2].
Population-Based Evidence: Low Yield in Asymptomatic Adults
A landmark study published in JAMA by Woolhandler et al. reviewed evidence from five population-based studies and found that "fewer than 2% of those with a positive heme dipstick have a serious and treatable urinary tract disease, too few to justify screening and the risks of subsequent workup" [3]. For proteinuria screening, the evidence was equally clear: "Proteinuria screening is not recommended in any asymptomatic adult population, since four population-based studies have found that fewer than 1.5% of those with positive dipsticks have serious and treatable urinary tract disorders" [3].
Infectious Diseases Society of America (IDSA): Recommend Against
The IDSA guidelines "specifically recommend against using pyuria or bacteriuria as a criterion for the diagnosis of UTI or for administering antimicrobial therapy" in asymptomatic individuals [2][4]. Similarly, "urinalysis results are not included in the National Healthcare Safety Network definitions of symptomatic UTI" [2].
The Problem with False Positives and Downstream Harms
One of the most serious concerns with routine urinalysis in general populations is the cascade of unnecessary interventions triggered by false-positive results. As Advani et al. described: "the widespread indiscriminate use of urinalysis, especially as screening tests in emergency departments, clinics, hospitals and nursing homes, has led to serious downstream consequences" [2].
The study documented that "abnormal urinalysis parameters in a patient without urinary symptoms is a powerful stimulus to order a urine culture and start antibiotic treatment, thwarting diagnostic and antibiotic stewardship interventions" [2]. This matters because patients treated with antimicrobials for asymptomatic findings were "not only unlikely to experience any reduction in risk of UTIs or surgical site infections, but also were more likely to develop adverse events like Clostridioides difficile infections" [2].
Furthermore, the dipstick urinalysis has inherent analytical limitations. Urine dipstick testing for proteinuria has a sensitivity of only 32 to 46% for detecting clinically significant levels of protein, meaning it misses the majority of cases where early kidney disease is present [5]. The test for nitrite has "poor sensitivity and specificity for diagnosing a UTI" and "a negative test for nitrite does not rule out UTI, as some urinary pathogens like enterococcus do not produce nitrite" [2]. Similarly, "varying thresholds of pyuria (WBCs >5/hpf vs WBCs >10/hpf) do not reliably predict bacteriuria or infection" [2].
Why Some Companies Include Urinalysis Anyway
Urinalysis is inexpensive and easy to perform, and some direct-to-consumer health testing companies list each urinalysis parameter as a separate "biomarker" to inflate their total test count. They count 20 urine parameters as individual biomarkers:
Urine Color and Appearance: These are subjective visual descriptions (e.g., "yellow," "clear," "cloudy") made by a technician looking at the specimen. They are not molecular measurements. Urine color reflects hydration status and can be altered by foods, medications, and vitamins. These observations do not provide actionable clinical data in asymptomatic individuals and should not be counted as biomarkers.
Dipstick Chemical Readings (qualitative, not quantitative): pH, Specific Gravity, Glucose, Protein, Ketones, Bilirubin, Occult Blood, Leukocyte Esterase, Nitrite, Microalbumin.
pH: Urine pH normally ranges from 4.5 to 8 and is heavily influenced by diet. "Urine pH is a measure of the acidity/alkalinity of urine and, by itself, usually provides little useful information. Under normal conditions its value is influenced by the type of diet (some diets: eg, diets rich in meat-having more acid content than others, eg, vegetarian diets)." [6]
Specific Gravity: This measures urine concentration, which is a marker of hydration status, not disease. "Specific gravity between 1.002 and 1.035 on a random sample is normal IF kidney function is normal" [7]. HealthieOne measures kidney function directly through BUN, creatinine, eGFR, and multiple specialized kidney markers, making urine specific gravity redundant as a screening tool.
Glucose: Urine glucose only becomes positive when blood glucose exceeds the renal threshold. "Glycosuria occurs when the filtered load of glucose exceeds the ability of the tubule to reabsorb it (i.e., 180 to 200 mg per dL)" [8]. This means a person's blood glucose could be dangerously elevated at 170 mg/dL and the urine dipstick would still read negative. Mayo Clinic Laboratory assessed urine glucose as having "Limited usefulness for routine screening or management of diabetes mellitus" [9]. HealthieOne measures glucose, HbA1c, 1,5-anhydroglucitol (1,5-AG), and three insulin resistance indices (TyG, TyG-BMI, METS-IR), detecting glucose dysregulation months to years before urine glucose would ever become positive.
Protein: The urine dipstick for protein has a sensitivity of only 32 to 46% for clinically significant proteinuria [5]. HealthieOne measures serum albumin, total protein, globulin, albumin/globulin ratio, and immunoglobulins (IgA, IgG, IgM) directly in blood, providing earlier and more specific detection of both kidney and systemic protein abnormalities.
Microalbumin: Microalbumin in urine is used to screen for early diabetic nephropathy. While this is the one urine test with some clinical value in specific at-risk populations (diabetics, hypertensives), professional guidelines do not recommend it for general population screening. HealthieOne measures serum albumin, eGFR, creatinine, BUN/creatinine ratio, cystine, and multiple kidney function markers that collectively detect kidney damage. If a HealthieOne Complete result indicates kidney concerns, your physician can then order targeted urine microalbumin testing as a focused follow-up.
Ketones: Urine ketone dipsticks use sodium nitroprusside, which "detects acetoacetate" but cannot detect beta-hydroxybutyrate (BHB), the most abundant and clinically significant ketone body. HealthieOne measures both beta-hydroxybutyrate and acetoacetic acid quantitatively in blood by LC-MS/MS, providing a more complete and precise assessment of ketone status than a urine dipstick that misses the predominant ketone entirely.
Bilirubin: Urine bilirubin is a crude qualitative indicator of liver or biliary disease. HealthieOne measures serum bilirubin quantitatively, along with ALT, AST, ALP, GGT, AST/ALT ratio, FIB-4 index, bilirubin-to-albumin ratio, and 15 individual bile acids by LC-MS/MS (including cholic acid, chenodeoxycholic acid, deoxycholic acid, ursodeoxycholic acid, lithocholic acid, and their glycine and taurine conjugates). This provides a molecular-level map of liver and biliary function that a urine bilirubin dipstick cannot approach.
Occult Blood, Urine: "Fewer than 2% of those with a positive heme dipstick have a serious and treatable urinary tract disease, too few to justify screening and the risks of subsequent workup" [3]. False positives occur with contamination, highly pigmented urine, strong oxidizing agents. HealthieOne measures hemoglobin, hematocrit, red blood cell count, reticulocytes, and reticulocyte hemoglobin equivalent in blood, providing far more specific information about red blood cell status and hemolysis than a urine dipstick that cannot distinguish between menstrual contamination, exercise-induced hematuria, and true pathology.
Leukocyte Esterase: "A positive test for leukocyte esterase may be seen in genitourinary inflammation, irritation from instrumentation or catheterization, glomerulonephritis, UTIs and sexually transmitted infections" [2]. It has "poor positive predictive value to diagnose infection" [2]. The IDSA guidelines "specifically recommend against using pyuria or bacteriuria as a criterion for the diagnosis of UTI or for administering antimicrobial therapy" in asymptomatic individuals [4]. HealthieOne measures white blood cell count, full differential (neutrophils, lymphocytes, monocytes, eosinophils, basophils, immature granulocytes), CRP, and multiple inflammation indices, providing a precise, systemic view of inflammation.
Nitrite, Urine: Nitrite has "poor sensitivity and specificity for diagnosing a UTI" and "a negative test for nitrite does not rule out UTI, as some urinary pathogens like enterococcus do not produce nitrite" [2]. False positives occur "on exposure to air or phenazopyridine, or from preanalytic contamination" [2]. This test only detects certain gram-negative bacteria and provides no value in asymptomatic screening.
Microscopic Sediment Findings
Red Blood Cell, Urine and White Blood Cell, Urine: These are counts of cells seen under a microscope, reported as number per high-powered field. "Hematuria is also not a reliable predictor of infection. Red blood cells may be present in other medical conditions such as acute glomerulonephritis, stone disease, trauma, malignancy, or menstruation" [2]. For white blood cells, "varying thresholds of pyuria (WBCs >5/hpf vs WBCs >10/hpf) do not reliably predict bacteriuria or infection" [2].
Bacteria and Yeast: Microscopic detection of bacteria or yeast in urine "cannot distinguish pathogens from nonpathogens or viable from nonviable organisms. Hence, detection of bacteria on the microscopic examination may be associated with positive urine cultures, but it cannot differentiate between asymptomatic bacteriuria, contamination, and UTI" [2]. Detection of yeast "is usually secondary to colonization of urinary tract, indwelling catheter, or vaginal flora" [2]. These findings are not clinically actionable in asymptomatic individuals.
Hyaline Casts, Urine: Only a few hyaline or finely granular casts may be seen under normal physiological conditions. Hyaline casts are commonly found in individuals after exercise or dehydration and are not indicators of disease. They provide no screening value in asymptomatic adults.
Calcium Oxalate Crystals: The presence of crystals in urine is influenced by pH, hydration, diet, and temperature of the sample. Crystal findings are common in individuals and do not diagnose kidney stones or kidney disease. HealthieOne measures serum calcium, phosphorus, uric acid, and kidney function markers (BUN, creatinine, eGFR) that provide far more meaningful assessment of stone-forming risk and kidney health than a microscopic crystal observation.
Amorphous Sediment: Amorphous sediment consists of unidentifiable particulate material seen under the microscope. It is a nonspecific finding and has no diagnostic value in asymptomatic adults. Counting this as a "biomarker" is misleading.
References
[1] U.S. Preventive Services Task Force. Screening for Asymptomatic Bacteriuria in Adults: US Preventive Services Task Force Recommendation Statement. JAMA. 2019;322(12):1188-1194. https://pubmed.ncbi.nlm.nih.gov/31550038/
[2] Advani SD, Polage CR, Fakih MG. Deconstructing the urinalysis: A novel approach to diagnostic and antimicrobial stewardship. Antimicrobial Stewardship & Healthcare Epidemiology. 2021;1(1):e6. https://pmc.ncbi.nlm.nih.gov/articles/PMC8486290/
[3] Woolhandler S, Pels RJ, Bor DH, Himmelstein DU, Lawrence RS. Dipstick urinalysis screening of asymptomatic adults for urinary tract disorders. I. Hematuria and proteinuria. JAMA. 1989;262(9):1214-1219. https://pubmed.ncbi.nlm.nih.gov/2668582/
[4] Nicolle LE, Gupta K, Bradley SF, et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clinical Infectious Diseases. 2019;68(10):1611-1615. https://pubmed.ncbi.nlm.nih.gov/31506700/
[5] Park JI, Baek H, Kim BR, et al. Comparison of urine dipstick and albumin:creatinine ratio for chronic kidney disease screening: A population-based study. PLoS One. 2017;12(2):e0171106. https://pubmed.ncbi.nlm.nih.gov/28152092/
[6] https://www.mayocliniclabs.com/test-catalog/overview/606510#clinical-and-interpretive
[7] Roxe DM. Urinalysis. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990. https://www.ncbi.nlm.nih.gov/books/NBK302/
[8] Simerville JA, Maxted WC, Pahira JJ. Urinalysis: a comprehensive review. American Family Physician. 2005;71(6):1153-1162. https://www.aafp.org/pubs/afp/issues/2005/0315/p1153.html
[9] https://www.mayocliniclabs.com/test-catalog/overview/609796
No comments yet. Be the first!